
The Complete Guide to Patellofemoral Pain Syndrome
Updated: 3/11/22
Key Points:
- What is patellofemoral pain syndrome (PFPS)? (13)
- Pain around or behind the patella, which is aggravated by at least one activity that loads the patellofemoral joint during weight bearing on a flexed (bent) knee (squatting, stairs, jogging, running, hopping and jumping)
- What is the prevalence of PFPS? (1,5)
- PFPS consists of 25% of all knee disorders in an orthopedic setting
- Common in runners and military, especially in youth during periods of rapid growth
- 3.8% of males and 6.5% of females get it annually
- What is the clinical presentation of PFPS? (1)
- Usually presents as a gradual onset of anterior (front) knee pain around or underneath the knee cap
- Generally hurts with movements that increase stress in the PF joint (squatting, stair climbing, hiking, running, prolonged sitting)
- What are the causes (mechanism of injury) of PFPS?
- There are several potential causes of PFPS including overuse, weak quadriceps, suboptimal movement, psychosocial factors (anxiety, fear of movement, depression), trochlear shape, body mass index and recovery (sleep, nutrition, stress) (2,17,18,19,21,22,23,25,26,27,40,41,43)
- What factors affect stress to the PFPS? (1,2,4,5,6)
- Surface area availability, (degree of knee flexion) joint reaction forces, quad contraction, patellofemoral compression and tracking
- How do you rehabilitate PFPS?
- Evidence Based Treatments for Patellofemoral Pain
- Progressively apply the appropriate amount of stress to the PF joint as well as the hip (2,13)
- Address causes of injury discussed prior (13,38)
Patellofemoral Pain Syndrome Definition and Stats:
What is patellofemoral pain syndrome (PFPS)?
Patellofemoral pain syndrome (or PFPS for short) is the most common knee condition treated in a physical therapy (or physiotherapy) outpatient clinics (1). PFPS is also commonly known as anterior knee pain, chondromalacia patella or runners knee.
PFPS is defined as:
- Pain around or behind the patella, which is aggravated by at least one activity that loads the patellofemoral joint during weight bearing on a flexed (bent) knee (squatting, stairs, jogging, running, hopping and jumping) (13)
- Additional criteria: Crepitus or grinding sensation emanating (coming) from the patellofemoral joint during knee flexion movements. Tenderness on patellar facet palpation, small effusion (joint swelling). Pain on sitting, rising on sitting, or straightening the knee following sitting. (13)
What is the prevalence of PFPS?
- PFPS consists of 25% of all knee disorders in an orthopedic setting (1)
- Common in runners, tennis, military (1,5)
- 3.8% of males and 6.5% of females get it annually (1)
- Seen more commonly in young adults and also occurs during periods of rapid growth (1)
What is the clinical presentation of PFPS?
- Occurs mainly in young adults especially during periods of rapid growth (1)
- Usually presents as a gradual onset of anterior (front) knee pain (1)
- Pain is usually present around or underneath the knee cap (1)
- Recalcitrant condition that can persist for many years without intervention (13). In other words this condition tends not to get better with rest and can stay painful for long periods of time.
- Generally hurts with movements that increase stress in the PF joint (squatting, stair climbing, hiking, running, prolonged sitting) (1)
- 75% of patients with PFPS present with tenderness along the patella (knee cap) (1)
- Tenderness on patellar facet palpation, small effusion (joint swelling). (13)
- Pain on sitting, rising on sitting, or straightening the knee following sitting. (13)
Anatomy of PFPS:
To understand PFPS it’s first important to have an idea of the relevant anatomy of the patellofemoral joint (PFJ). The PFJ consists of the patella (also commonly known as the knee cap) and the femur. (4)
The PFJ is the connection between the patella and femur (patello-femoral). The patella sits on the front of the femur and slides along this bone on something called the “trochlear groove” The patella sliding along the groove is often explained as a train (the patella the train tracks (trochlear groove) . (4)

Source: Attribution: Jmarchn / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0) Edited by fitness pain free LLC
As we descend down into a squat (or descend stairs, lunge etc.) the knee cap engages into the trochlear groove (track) and is guided down the femur. As we straighten the knee (coming up from a squat) the patella tracks back up the groove. We call this patellar tracking. When doctors speak about patellar tracking (or mal-tracking) they’re discussing this phenomenon. (4)
The inside of the PFJ is covered in articular cartilage, which is a tough connective tissue (15) designed to buffer the stress that occurs in the joint created by the quadriceps (more on this later).
One of guiding principles of PFPS is that if we do not have proper alignment of the patella in the trochlear groove we can end up with increased stress within the PFJ (mainly on the outside or lateral part of the joint) and pain. This is known as “mal-tracking” (4).
Side Note: I’m getting ahead of myself here but I want to make sure you understand that having tracking issues in the knee is only 1 piece of the equation of PFPS. The causes of PFPS are multifactorial but tracking is one piece of the puzzle. Read on for the rest of the story .
Within the PFJ there are a variety of structures that can get irritated. These structures are (1):
- Synovial plicae
- Infrapatellar fat pad
- Retinaculae (medial or lateral)
- Joint capsule
- Patellofemoral ligaments
- Subchondral bone (bone underneath of the cartilage)
- Prolonged stress to the PFJ could lead to increased cartilage degeneration (wear and tear) (1)
There are also a variety of structures within the knee that help with alignment and patellar tracking of the PFJ. Some of these structures are known as “passive structures” and some as “active structures”. Active structures refer to muscles that can actively contract and and help stabilize the PFJ in that manner.
Passive structures are non-contractile in nature and refer to things like ligaments and boney structure. They add to the inherent stability of the joint, but they can not contract and we generally can’t alter these structures through rehabilitation (although surgery can help in this regard) (4).
Passive structures that stabilize the PF joint (4):
- Boney alignment of the patella and trochlear groove (a more shallow groove increases the risk of patellar subluxation) (4).
- Patellar tendon
- Joint Capsule
- Medial meniscopatellar ligament
- Medial retinaculum
- Medial patellofemoral ligament
- Lateral patellofemoral ligament
- Iliotibial band (IT Band)
- Lateral retinaculum
Active structures that stabilize the PF joint:
- Quadriceps (special emphasis on what’s called the “VMO” or the oblique fibers of the quadriceps muscle called the vastus medialis. These fibers attach directly to the patella and directly help control the medial (inside) of the knee joint.
- Pes anserine muscle group (adductor / hamstrings group: semitendinosus, gracilis, sartorius)
- Biceps femoris (part of the hamstrings muscle group)
All of these structures play a role with the tracking of the PF joint and will become important as we discuss PFPS rehabilitation in the next few articles.
Local Structures that Support the Patellofemoral Joint
Next I’d like to discuss some of the local structures. The surrounding joints are actually really important when understanding PFPS and how to treat it. One saying I really find true is,
“the knee is a slave to the joints above and below it.”
What I mean by this is that what occurs in the knee joint (patellar tracking specifically) is heavily influenced by both the foot (subtalar and mid-foot joints), ankle (talocrural joint) and hips. I want to briefly touch on some of the anatomy of these structures and their importance will become much more relevant when we go over the biomechanics of PFPS soon.
The Hip
The hip is a very large joint with several equally strong muscles that influence the PF joint indirectly.
- Glute medius
- Glute maximus
- The deep hip lateral rotators (Piriformis, gemellus superior, obturator internus, gemellus inferior, quadratus femoris and the obturator externus)
The glute muscles of the hip attach directly to the femur thus playing a direct role in the tracking of the PF joint as well as the total amount of stress the joint takes when we move around. Strengthening these muscles also helps to eliminate pain during PFPS. (2)
The Foot and Ankle
The talocrural joint:
The talocrural joint is responsible for both dorsiflexion and plantar flexion. The reason why total ankle dorsiflexion is important is because the amount of dorsiflexion present in our ankles will partially determine how much knee flexion (bending) occurs when we perform movements like squatting and running.
As we’ll see later, knee flexion has a direct correlation on how much stress the PF joint takes with our movement. Limited ankle mobility can also play a role in patellar mal-tracking. The total amount of motion at this joint is influenced by both our gastrocnemius and soleus (calf) muscles, as well as the joint itself. This has important considerations because we'll most likely be targeting this area in folks with stiffness affecting the PF joint.
The subtalar and mid-foot joints:
These joints have a direct influence on how much of an arch we have in our feet. This is important because the arch in our foot influences the amount of rotation that occurs in our tibia (shin bone). The tibia attaches directly to the patellar tendon (which attaches to the patella). Motion at the subtalar joint will affect patellar tracking. Some of the major structures that help to control the arch of the foot are:
- Gastrocnemius and soleus (calf) muscles
- Tibialis posterior
- Flexor hallucis longus
- Subtalar and mid-foot joints
To recap thus far:
- PFPS is the most common source of knee pain seen in physical therapy outpatient clinics
- PFPS is defined as: Pain around or behind the patella which is aggravated by at least one activity that loads the patellofemoral joint (squatting, stairs, jogging, running, hopping and jumping) (13)
- The patella tracks along a groove during knee flexion
- The alignment of the patella in it’s groove is important and if this is altered it can lead to irritation of several tissues in and around the PF joint
- There are both passive and active structures that control stability and alignment of the PF joint. Control from these structures is vital to health of the joint .
- The knee joint is heavily influenced by what’s occurring at both the hip as well as the foot. Stress in the PF joint can be increased or decreased by affecting these joints (more on this later).
Now that we got the basics out of the way we can start diving into the good stuff. There are 2 major bio-mechanical factors to understand that occur during PFPS:
Biomechanical Considerations:
When we perform movements like squatting, running and stairs the patellofemoral (PF) joint takes stress. It’s important to understand this concept. No matter how perfect our technique is or how strong we are the PF joint will take stress during these movements. Also keep in mind that this joint was made to handle this stress and has very durable cartilage to help handle the forces of your activities.
However, sometimes when there is too much stress knees can become painful. This is a central concept of PFPS. Therefore it makes sense that we should have some sort of awareness of what activities and motions create more or less knee stress. Lucky for us, the amount of stress in the PF joint can be measured so we can get an idea of just how much stress the joint takes and which movements create the most (or least) stress to the joint.
1: Surface Area Availability
There are 2 things to understand when discussing stress in the PF joint. The first is the amount of total surface area available in the joint to dissipate force. Before we get into this subject I wanted to first have a little discussion on surface area and stress .
A central concept to understand is that a larger surface area dissipates force more easily than a smaller surface area. In other words, the same force applied to a large surface area is less force per square inch than that same force to a smaller surface area.
Here’s another way to think about it. Let’s compare being punched by a fist vs. being punched with a knife. The surface area of the fist is broad and when it hits your shoulder it may hurt but probably won’t cause much damage. Let’s contrast that with the knife. If the knife hits your shoulder with the same force, the surface area of the pointy knife is so small it would go right through your shoulder, causing quite a bit of damage.
Small surface area (knife) = hard to dissipate force
Broad surface area (fist) = easier to dissipate force
Based on this rule, having a large surface area to dissipate force in the knee is good. However, the amount of surface area available between the patella and femur to dissipate force during movement is variable depending on how much the knee is bent.
When the knee is fully straightened there is actually no contact (surface area available) of the femur against the patella. When we first start to bend our knees, in the first 20 degrees of motion the patella begins to engage the femur.
Initially there is very little boney contact between the two structures. However, as the knee starts bending further there is more and more contact (surface area) between the patella and femur. The surface area of contact continues increasing until about 90-120 degrees of knee flexion. At this point the surface area actually begins decreasing as we approach full knee flexion (2) .

So this point is fairly complex to understand so we’ll re-cap below (2):
- 0 degrees knee flexion = no contact between patella and femur
- 0-90 degrees of knee flexion = surface area contact steadily increases (**Wrapping effect begins at 70 degrees)
- ~90 degrees knee flexion = maximal surface area contact between patella and femur
- 90-135 degrees knee flexion = surface area contact decreases
- >135 degrees = surface area contact continues to decrease and is lowest at end range knee flexion
**Side Note: To make matters a bit more confusing, as the knee flexes past 70 degrees the quadriceps tendon comes into contact with the femur. This also serves to increase surface area contact within the patellofemoral joint potentially increasing surface area available to dissipate force. This is known as the “wrapping effect”. This wrapping effect may potentially help to dissipate forces as we descend to depths below 70 degrees, however there is not much research to either support or refute this claim.
So here’s the thing. Increased surface area between the patella and the femur is a good thing. More contact gives more area to dissipate forces within the joint. Therefore, around 90 degrees of knee flexion there should be the least amount of stress through the knee joint right? We should all perform our squats to 90 degrees of knee flexion to minimize stress on the knee?
I wish it were that simple…
2: Joint Reaction Forces and Quadriceps Contraction
The second principle to understand are joint reaction forces and quad contraction. Basically the more the knee goes into flexion (knee bending) and the harder the quadriceps contracts, the greater the forces on the patellofemoral joint.
So, despite the surface area of the joint increasing as we descend to 90 degrees of knee flexion, the PFJ forces increase substantially and are not off-set by the increased surface area of the joint (2).
Food for thought: From an evolutionary perspective maybe our knees developed more surface area around 90 degrees of knee flexion in an attempt to buffer some of the increased stress that comes from loaded knee flexion .
Activities that take us into more and more knee bending tend to stress the knee more and more. We have some research to show how much stress goes through the PF joint during several different activities (4). Notice that activities that require more knee bending tend to place larger stresses through the PF joint:
- 1.3 times body weight during level ambulation
- 3.3 times body weight during stair ambulation
- 7.8 times bodyweight during a deep knee bend or squat
Now PFPS is largely thought to occur from overuse of the PF joint. From this graph it can be pretty easy to see why squatting can create knee pain if abused and why stairs can be irritating once PFPS has started. This also helps to explain why those who perform a lot of deep squatting are susceptible to knee pain.
Decreased surface area contact at bottom of squat + high quadriceps contraction = Lots of PF joint stress
I’m not saying to stop squatting but I am saying it makes a lot of sense why these athletes get painful knees from time to time, especially given that adding load to the squat also increases stress on the PF joint (16).
Side Note: For this discussion we’re describing how the joint takes forces during closed chain activities like squatting, running and stairs. These principles are not the same when we stress the joint in an open chain fashion (when the knee is fixed and the foot swings freely, like a seated knee extension). Lucky for us, most of the movements we perform in life and in the gym that load the PF joint are performed in this closed chain fashion.
4: Patellofemoral Compression
Another factor that can increase stress in the PF joint is tightness of the quad musculature (1). This is documented as a patellofemoral compressive issue (1). The quadriceps muscle attaches directly to the knee cap and then the knee cap attaches directly to the tibia. This forms a strap.
As the knee flexes further and further the strap tightens and compresses the patella into the trochlear groove causing compression within the PF joint. This is potentially the reason why patients with PFPS also have pain with prolonged sitting. They’re just sitting in a position which compresses the joint for a long period of time and can eventually cause pain. (movie theatre sign)

Patients with PFPS have also been shown to present with increased tightness of their quads and hip flexors (through thomas testing), as well as tightness in the IT band (Ober testing) (1). Restoring normal flexibility (Thomas and Ober tests) in those areas has been shown to be a predictor of recovery from PFPS (1) .
5: Patellar Tracking
So in part 1 of this article series we discussed the trochlear groove of the femur and how the patella fits into this groove. As the knee bends the patella tracks down along this groove in the femur. Like we spoke about earlier, having optimal alignment of the patella in the groove is important for the health of the joint. This alignment allows greater surface area of the joint to dissipate forces and ensures the forces are spread evenly throughout the joint. Several factors can effect this tracking and we’ll discuss these below.
Issues from the Knee
From earlier in the article we spoke about one of the passive stabilizers of the knee being the boney fit of the patella into the trochlear groove. The better the fit, the easier tracking is.
It’s important to understand that this fit is variable and not as good from person to person (4). Unfortunately this is not something that we can fix with surgery and these folks sometimes have trouble with dislocation of the knee cap (which is a topic for another discussion). Check out these different variations of trochlear grooves below:

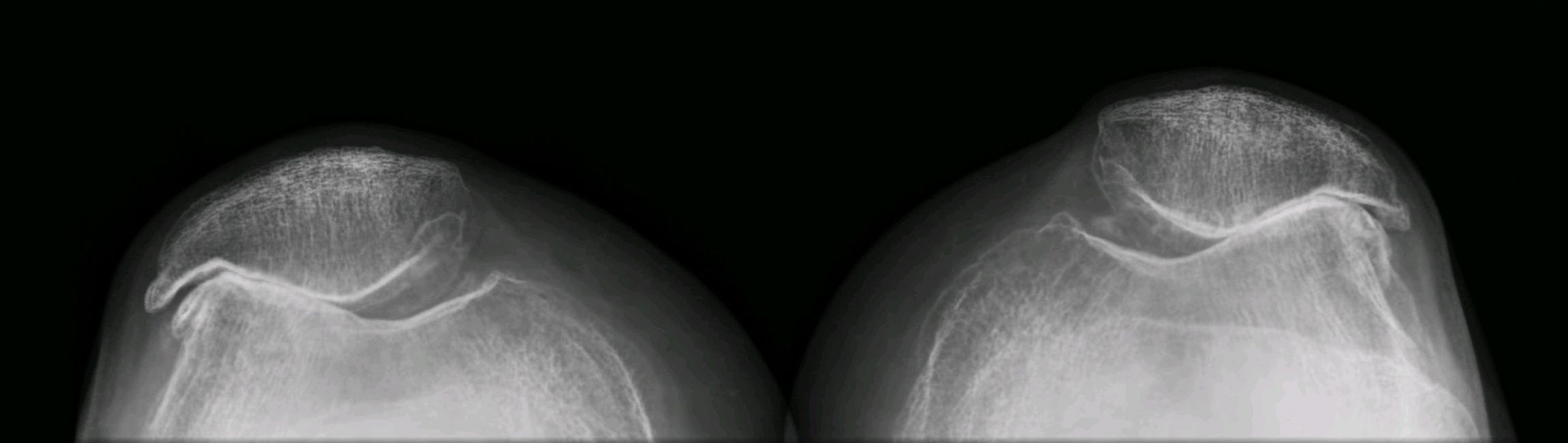{kind=link}
Unfortunately, people with a hypermobile patella have been shown to be at increased risk of developing PFPS.
In PFPS there is generally increased stress to the lateral (or outside) portion of the PF joint. This will occur for a variety of reasons but one potential cause for this can be tightness on the lateral (outside) portion of the leg. These potentially tight structures include:
- Lateral patellofemoral ligament
- Iliotibial band (IT Band)
- Lateral retinaculum
Tightness of the IT band pulls directly on the patella through the lateral retinaculum. This is theorized to pull the patella laterally (to the outside of the body) and cause mal-tracking. This increases stress to the lateral side of the joint (1). Fortunately as we’ll discuss later, normalizing this flexibility has been shown as a predictor of those who rehabilitate from PFPS (1) .
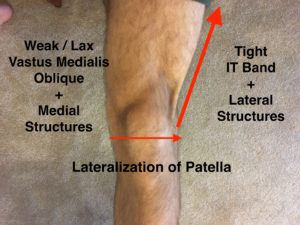
Keep in mind that it isn’t just tightness on the outside of the leg that can produce issues. We could also have looseness, weakness and or timing issues of the medial stabilizers. Looseness or weakness of these structures can cause the knee cap to track laterally in it’s groove during exercise. Some of these structures are the:
- Joint Capsule
- Medial meniscopatellar ligament
- Medial retinaculum
- Medial patellofemoral ligament
- Quadriceps (VMO)
- Pes anserine musculature
- Biceps femoris
Remember that the vastus medialis oblique is an active medial stabilizer of the knee. Individuals with PFPS tend to have delayed firing of the VMO. A lack of control from this muscle which could alter patellar tracking (8). We also have some research to show that altered firing times of the VMO can predict people who go on to develop PFPS. (although this research is mixed)
Just keep in mind again that this is simply one factor in a large group of variables that can influence stress in the patellofemoral joint. Due to mixed research on VMO firing in folks that have pain vs. no pain, the inability to target the VMO with exercise and the improbability of being able to actually stretch and loosen the IT band, this current theory for the development of PFPS is hotly debated and challenged.
Issues from the Hip
As we discussed earlier the muscles of the hip help to control motion at the femur. One motion they help to control is internal rotation of the femur. If we lack control of the hip the femur can fall into internal rotation.
Some studies have shown that individuals with PFPS have increased hip femoral internal rotation (5, 6). The reason why this is not ideal is because it can alter patellar alignment and cause lateralization of the patella, increasing stress to the lateral side of the joint.
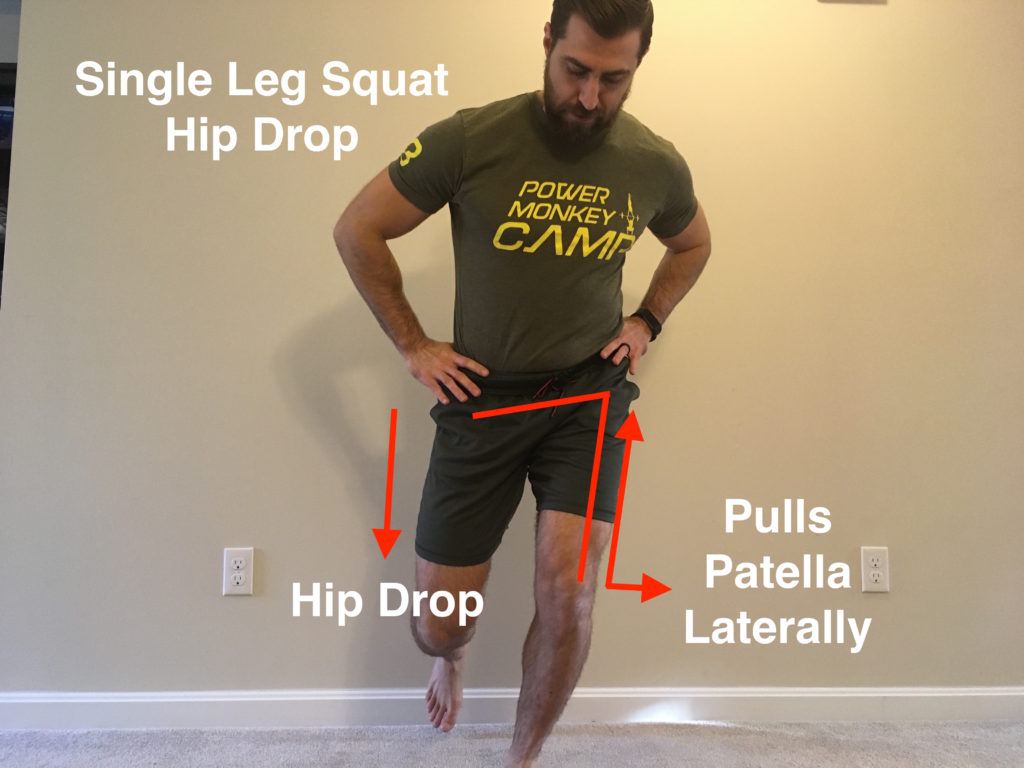
Femoral internal rotation also reduces contact area of the PF joint. Remember how more surface area is generally good and less surface area increases PF stress? If we’re lacking control of femoral rotation, we’re increasing stress on the PF joint by decreasing surface area and placing more stress on the lateral side of the joint. This can happen during movements like squatting, running, lunging and stair climbing. Below you’ll see me performing a single leg squat, first with optimal alignment (I'm trying my best!).
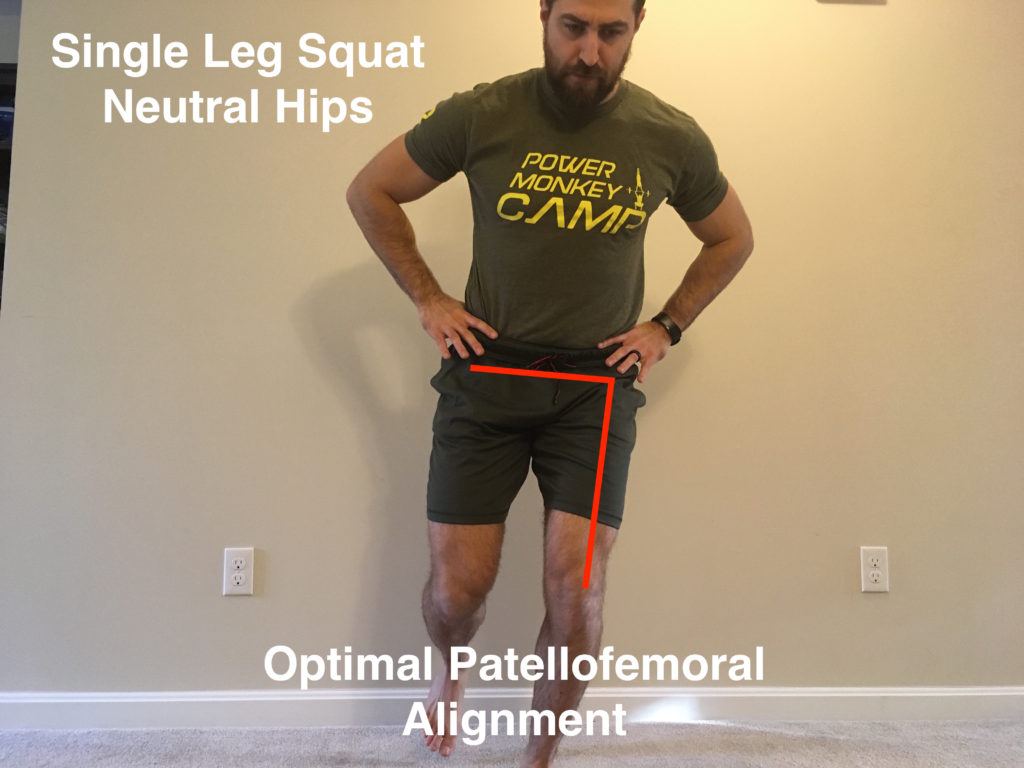
When the angle between the hip and pelvis is neutral (90 degrees as seen above), we’re setting ourselves up for optimal alignment of the PF joint.
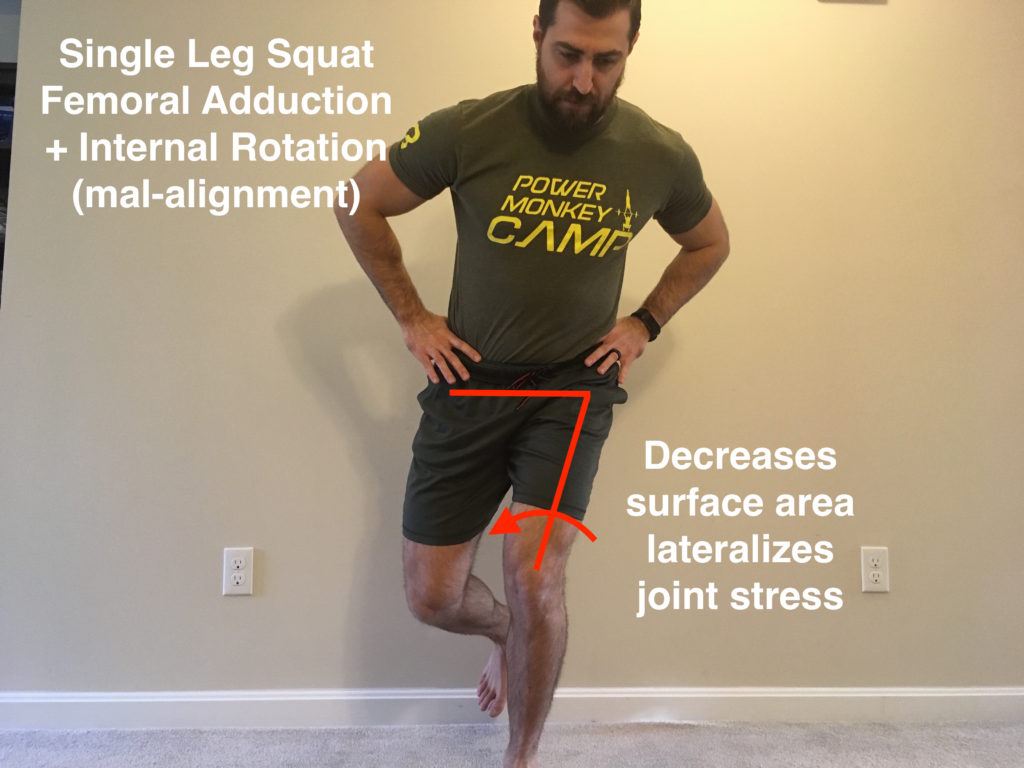
In this demonstration you can see how the hip comes toward midline (adduction) and the femur internally rotates. When the hip comes toward midline (adduction) or the opposite hip drops (same motion except now the pelvis is moving and not the femur) we also get some issues downstream at the knee. Observe below:
As the opposite hip drops it will stretch the TFL and glute musculature, both of which attach to the IT band. The IT band attaches to the lateral retinaculum and again, pulls the patella laterally. Increased hip internal rotation and adduction is a risk factor associated with PFPS (4). Females with PFPS consistently have weaker hip extensor, abduction, external rotation strength (4). This weakness also correlates with hip adduction and internal femoral rotation with activity (stair descent, running, cutting, jumping) (4).
If we don’t control either femoral adduction or internal rotation, we may be setting ourselves up for knee problems. Now you can see why the hip is so important.
Issues at the Foot / Ankle
On the other side of the knee we’ve got the good old foot, ankle and tibiofemoral joint. Before we talk specifics, let’s start by understanding the movements at these joints better. These movements are a little tough to wrap your head around so Ive made some handy videos and images to help illustrate the major points:
In the video above you’ll find foot pronation and supination.
In the video above you’ll see tibial rotation (yes the knee is meant to rotate some).
In this video you have tibial rotation in closed chain. This is essentially the same movement as the video prior except the foot is now fixed to the ground while the hip rotates. Closed chain tibial rotation is more important because most of the movements we perform in our lives and training occur in closed chain (stairs, squatting, lunges etc…).
As we explained earlier, the tibia attaches directly to the patella via the patellar tendon. When we externally rotate our tibia the attachment point of the patellar tendon goes laterally. Now when we flex the quad the angle of pull will be directed laterally. Check out the video below to get a better idea of what’s occurring here.
Now the most obvious way to tell if someone is squatting, running or jumping with excessive tibial rotation is to look at where the knee cap is facing in relation to the foot. Check out the video below and notice how the toes are not facing the patella during the squat:
Now it makes sense that if we’re sitting in external rotation when we perform knee bending tasks we’re lateralizing stress to the PF joint. Again, this decreases surface area within the PF joint and increases stress to the lateral part of the joint.
The next concept to understand is that what happens at the foot will affect all of the joints above the foot. Most importantly, foot pronation can cause femoral internal rotation. Recall that femoral internal rotation alters patellar tracking. Check out the image below to see what I’m talking about:
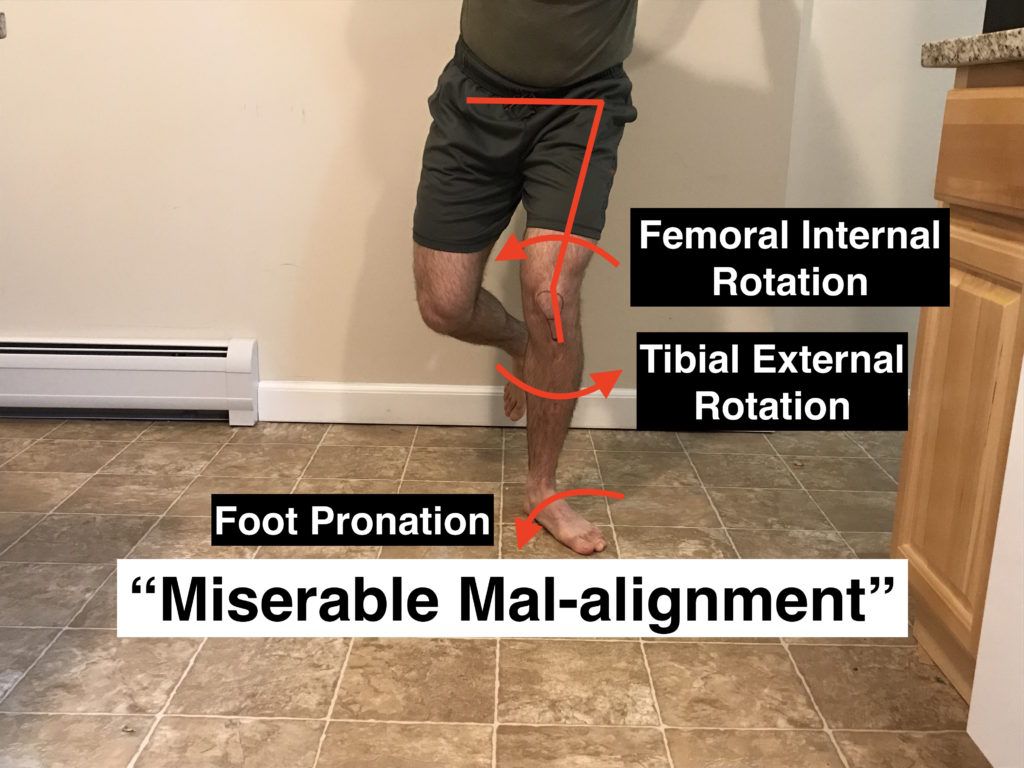
As the foot falls into pronation, the entire chain follows. They’ve even named the combination of foot pronation, tibial external rotation and femoral internal rotation “Miserable Mal-alignment” because of it’s effects on the knee. Although it is maybe a little harsh describing this condition as “miserable” it does help to illustrate the point. You can certainly now see how excessive motion at the foot and ankle can cause issues at the knee .
Next we’ll take a closer look at the ankle. The ankle actually has 2 main joints that allow motion. The first we already alluded to. It’s called the subtalar joint and controls pronation in the foot. If we have too much pronation this leads to femoral internal rotation of the hip. The other joint is called the talocrural joint. This is the joint responsible for dorsiflexion and plantarflexion of the foot:
Activities like squatting, lunging and even running require a pre-requisite amount of dorsiflexion. The trouble is, not everyone has the required amount of ankle dorsiflexion to perform these movements. However, the body finds a way to perform these tasks if we ask it to. What ends up happening in this situation is that when we run out of talocrural range of motion, we’ll start compensating with motion from the subtalar joint (pronation) and with tibial external rotation. I made a video several years ago (with an accompanying article) to help illustrate this point better:
What we end up with is “toe out” or “knee in” as we descend into a squat. Check out the video below to see this in action:
Now this can also occur during squatting tasks using 2 legs. Observe the image below:
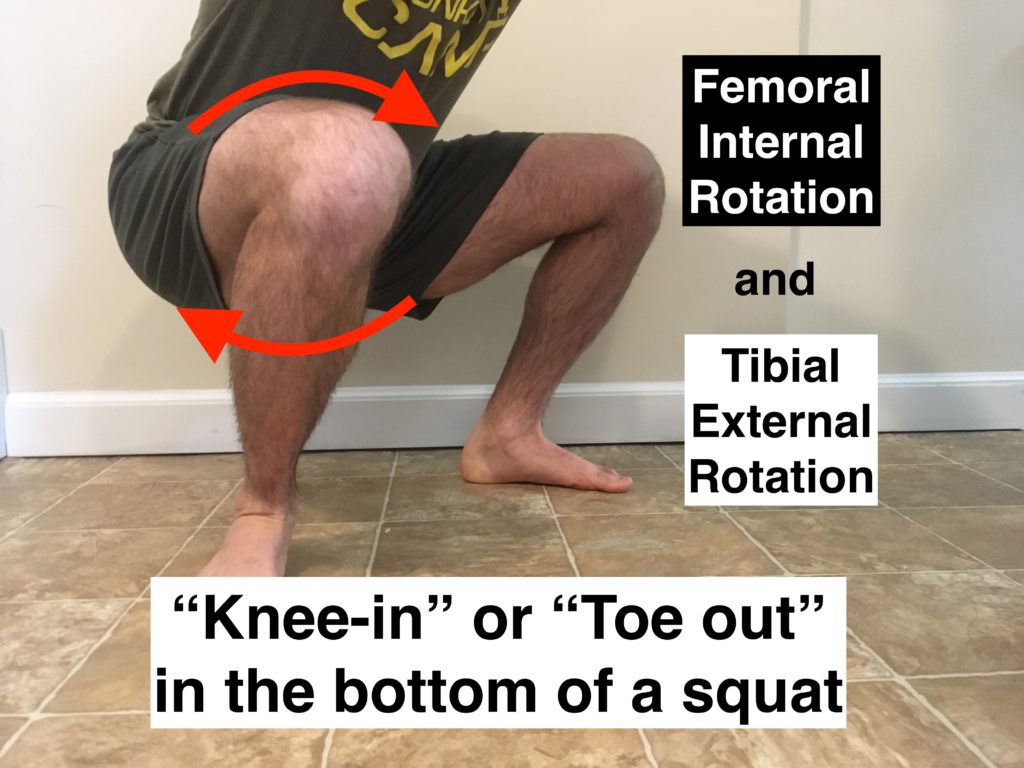
If you’ve been squatting or observing other squat for long enough I’m sure you may have seen this situation. Since the PF joint forces are already very high in the bottom of a loaded squat, having poor motion at the foot or hip definitely doesn’t help the situation.
Just keep in mind that in a deep squat pronation, tibial rotation and hip internal rotation can be major players in this pattern. However, a lack of adductor mobility can also potentially drive this problem too.
Side Note: I know I just made an enormous case for “poor movement ” at the hip, tibia and ankle as drivers of patellofemoral pain syndrome. I think it’s important to note that not all people with PFPS move with poor mechanics. Only 50% of people with PFPS move “poorly” as shown by Chris Powers’s (2) research. The evidence is also mixed as to whether or not poor movement leads to PFPS. Some studies support it and some others do not. It does however seem that after people develop PFPS they tend to move differently (10) (and show more of the characteristics described in this article). We’ll discuss some other potential drivers of pain in future articles .
So to recap:
- Patellofemoral pain syndrome is largely a condition of overuse
- Poor patellar tracking can increase stress within the PF joint
- Activities with increased knee flexion increase stress to the PF joint
- Increased load and quadriceps contraction increases stress within the PF joint
- Looseness or weakness of structures on the medial (inside) side of the knee joint can affect patellar tracking
- Tightness of structures on the lateral (side) or anterior (front) of the knee joint can increase compressive stress in the PF joint
- Patellofemoral pain syndrome can be influenced by the joints above and below the knee
Capacity and the Patellofemoral Joint
Going back to our previous point, PFPS is largely described as an issue of overuse (4, 11). If we get too much stress within the patellofemoral (PF) joint we can create some tissue irritation and as a result end up in pain. They key point here is the issue of “too much” stress. Again remember that the knee is designed to handle stress and that in general movement and exercise is good.
As described, certain activities place more stress on the PF joint than others. Activities like running and deep squatting can place large forces on the PF joint. Because of this PFPS is a common injury seen in runners and weightlifters .
Also remember how certain biomechanics of the hip, knee, foot and ankle all play a role in knee pain. If biomechanics are off, we run into decreased surface area in the PF joint to dissipate force as well as more stress on the lateral (or outside) portion of the joint.
Basically, suboptimal movement at the patellofemoral joint increases stress on the joint. Just keep in mind that stress isn't a bad thing, it can actually be quite beneficial to cause the joint to adapt over time. In order to understand this better we'll discuss patellofemoral "capacity".
Tissue Homeostasis
Scott Dye is a famous knee researcher who first discussed the topic of “tissue homeostasis” and capacity of the PF joint. Wikipedia defines homeostasis as:
Homeostasis can be defined as the stable condition of an organism and of its internal environment; or as the maintenance or regulation of the stable condition, or its equilibrium; or simply as the balance of bodily functions.
Basically the PF joint is attempting to maintain it’s homeostasis like any other part of the body. Scott believes that a single insult or a period of prolonged loading to the PF joint can alter the joint’s homeostasis and create knee pain (11).
Envelope of Function
Scott described the knee’s ability to handle stress (the capacity of the PF joint) as the joint’s “envelope of function” (11). Basically, the knee joint can handle a certain amount of stress prior to it becoming injured and or painful. If we exceed this capacity then we end up with knee pain.
Let’s look at 2 examples below. One is a beginner lifter who just became interested in weight training and wants to start a beginner weightlifting program. In the image below the area in grey represents what the lifter’s knee is capable of handling before an injury occurs. The area in the white represents what the knee is not quite capable of and can cause injury:
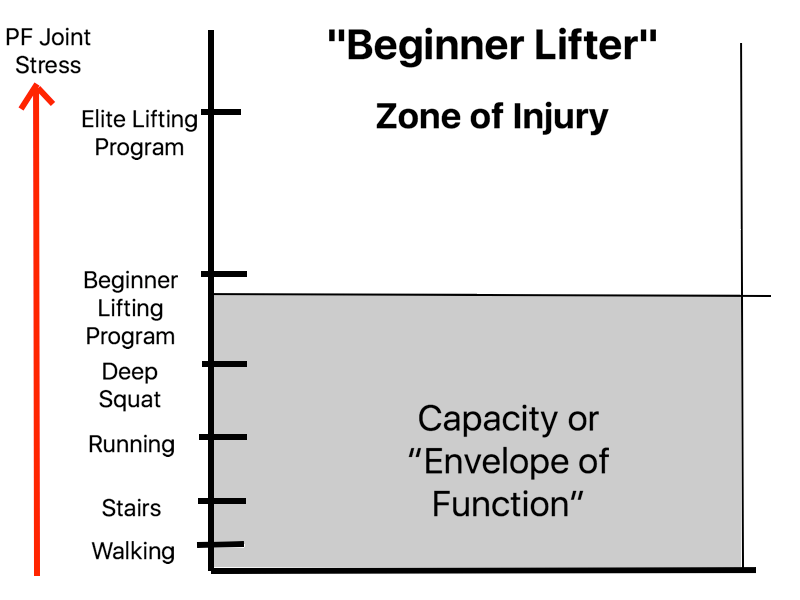
As you can see this individual can perform stair climbing, squatting and running without any pain. All of these activities are within their envelope of function. However, they’re not quite ready to start a beginner lifting program. That’s right above their envelope of capacity. Put them into an elite training program and they’re gonna have some pretty angry knees .
What’s very interesting about the PF joint is that it seems we can increase the capacity of the knee joint with training over time. The greater the capacity of the joint, the greater tolerance we have before experiencing pain. This is potentially why you can have athletes who can perform a large volume of running or loaded deep squats throughout a training week and never experience any pain. They’ve built their capacity for it over time. If you give the same training load to a coach potato then you’ve probably just injured someone.
For the athlete depicted in the graph above they will require a period of training to increase their capacity prior to beginning a true program. Let’s imagine that we take the same lifter and train them over the course of 10 years. Now they’re an elite weightlifter. Their envelope of function has improved.
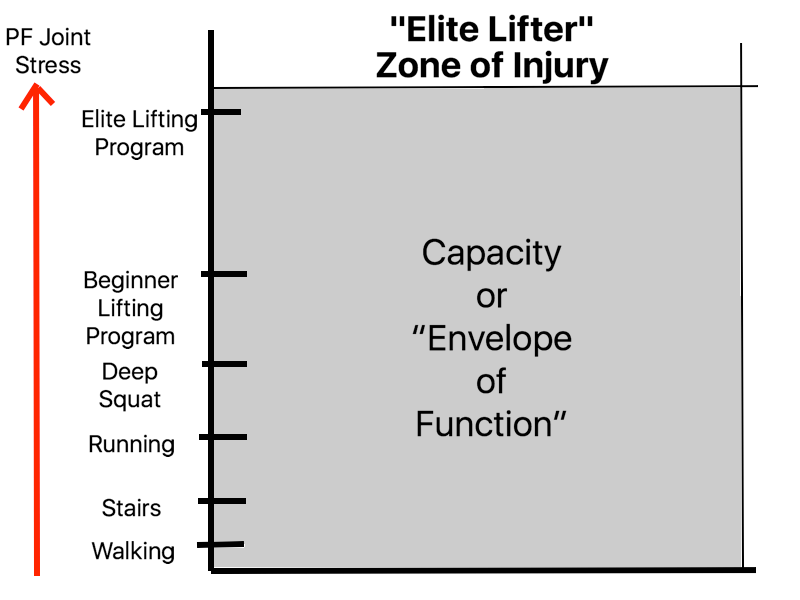
Our weightlifter has been building the capacity of the knee joint over the course of years and they are now able to handle much more volume, intensity and frequency of loading to the PF joint than when they started. Even though the stress on the PF joint is far higher in the elite lifter’s program their capacity has risen to match this stress. Therefore they continue to train within their envelope of function and maintain the homeostasis of the joint .
Now, what happens when 2 elite athletes run the same race and only 1 gets hurt? Well this can be simplified with the images below. Look at running athlete “A” below:
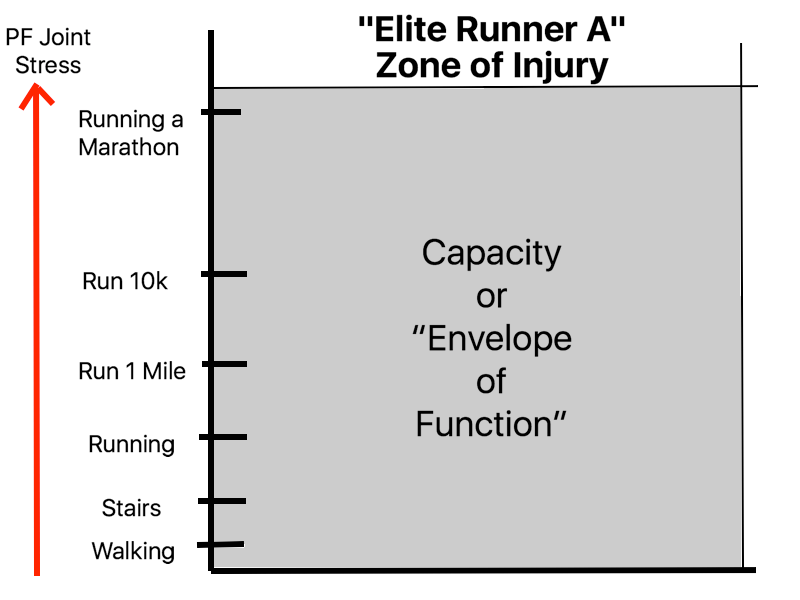
They have enough capacity to handle races up to marathon distance without getting injured. Let’s contrast this to athlete “B”
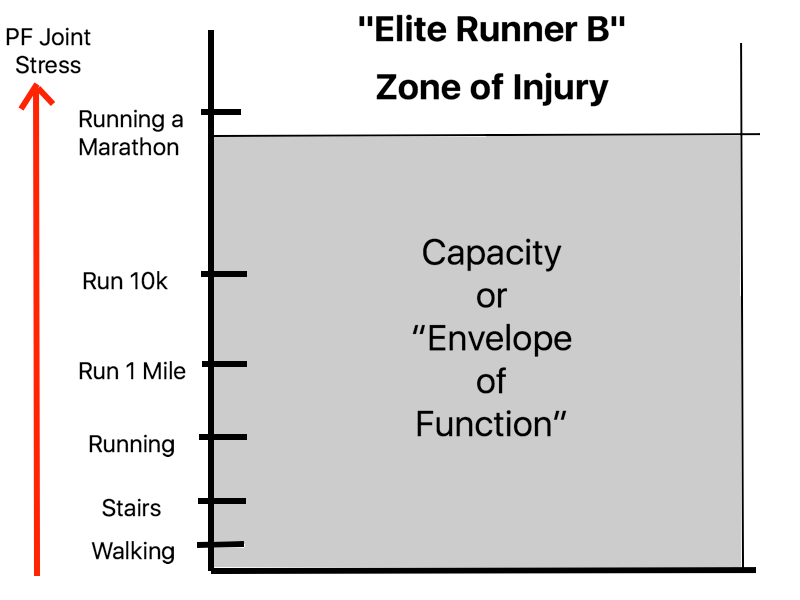
In this example our running athlete can handle most running distances below a marathon. Theoretically, once they decide to try a marathon they would end up in pain. The race exceeded her capacity and resulted in knee pain.
So to recap:
- Patellofemoral pain syndrome is a condition of overuse
- An initial insult of overuse can disrupt the “homeostasis” of the PF joint and lead to indefinite length of pain unless intervened upon
- PF joint capacity is the amount of stress the knee joint can handle before an injury results
- PF joint capacity can be increased (or decreased) depending on the stress placed on the joint with training and regular activity
- PF joint capacity helps explains why certain athletes get injured and other don’t
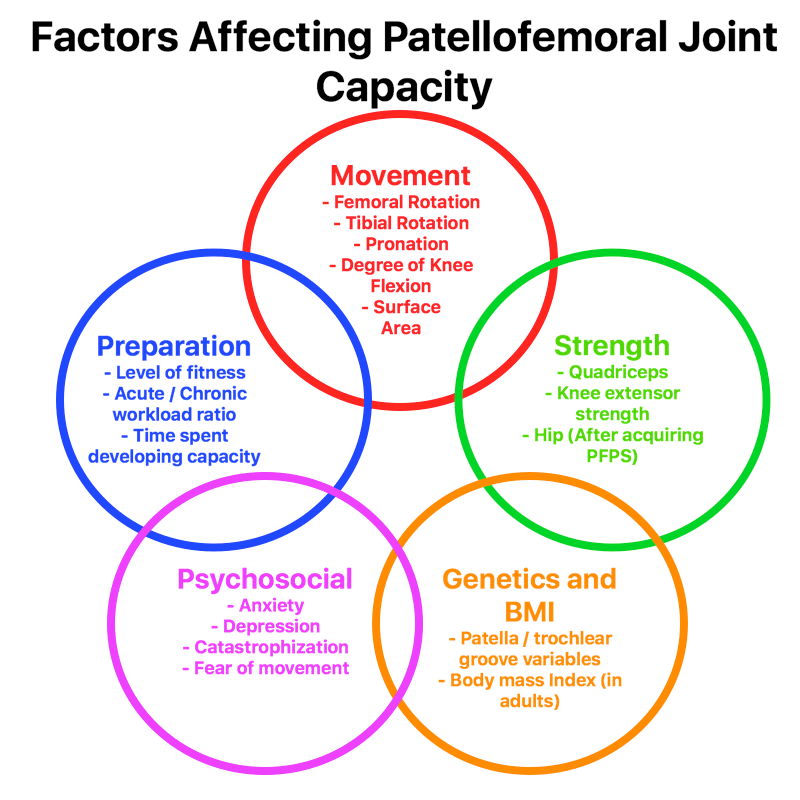
Factors that Influence Risk of Injury
- Preparation
- Strength
- Movement Quality
- Psychosocial Factors
- Genetics and BMI
- Recovery
Now as you might have guessed, PF joint capacity is going to be influenced by a variety of factors. This capacity is going to be very important in both determining how much the knee will be able to handle before it becomes painful and how much stress will be beneficial to the knee after an injury for rehabilitation.
1: Preparation
We have quite a bit of newer research coming out showing that a very large predictor of injury is training volume. If we go over a certain threshold of training volume, our risk of injury goes up (17, 18, 19).
One particularly promising area of injury prediction research is looking at spikes in an athlete’s training volume (20). Most of this research is coming from Tim Gabbett who has studied rugby and soccer (football) athletes. Spikes in training volume are defined as any event of training that far exceeds the typical volume of training .
It makes total sense, do way more than the body is accustomed to, we get hurt. Tim calls this the acute to chronic workload ratio.
Basically if the acute training load (the total volume of training performed in a given week) is much larger than the chronic training load (average training volume over the past several weeks) then we’re more likely to get hurt (17, 18, 19, 20).
A few examples:
- The athlete who begins a squat program on top of their normal training (doubling training volume) and gets knee pain
- The athlete who begins adding running intervals into their program 2x per week in addition to their normal training (doubling training volume) and gets knee pain
Here’s the kicker, what Tim also found was that high levels of volume are actually predictive of lower risk of injury (20).
Tim found that athletes with higher VO2 max (a marker of cardiovascular fitness) and had longer preseasons were less likely to get hurt (17, 18, 19). Basically athletes who had greater fitness and longer periods of preparation before their competitive season began were less likely to get hurt.
Athletes who were accustomed to handling a large volume of training were less likely to be injured. This makes sense, athletes that train at a higher volume are potentially more adapted toward higher training volumes. They are potentially creating greater “capacity” to handle these training loads and less likely to be hurt when exposed to higher volume training environments (tournaments, multi-day competitions etc.). Remember the olympic lifting athlete described earlier. She was able to increase her capacity over time to handle much larger training volumes without getting hurt .
We can take these same concepts and apply it to our injury prevention tactics. Slowly increasing training volumes over time can increase our capacity and make us better able to handle larger and larger amounts of stress. Throw too much at our athletes too soon and risk injury.
2: Strength
Far and away the greatest predictor of having future patellofemoral pain syndrome is having weakness with knee extension or weakness of the quads (2, 21, 22). People with PFPS have been shown to have a 6-12% deficit in strength compared to healthy controls without PFPS (2). This makes sense, if the quadriceps are not capable of handling the stress of a given activity, the knee becomes painful. It also seems that having PFPS creates (or increases) weakness.
Patients with PFPS tend to have weakness in the hip musculature as well(abduction, extension, external rotation) (4). Patient with PFPS also present with reduced lateral core strength (9). These reductions in strength also tend to correlate with dynamic valgus seen in single leg squat tasks (4).
Side Note: What’s interesting is that weakness of the hips (abduction and external rotation) is NOT a predictor of future PFPS (21, 22). Some research actually shows those with great hip strength have an increased risk of PFPS (2). It seems that weakness of the hip only occurs after already acquiring PFPS (21, 22).
It makes sense that having weakness of the hip could create poor movement during squatting and jumping maneuvers and thus PFPS but just keep in mind that the research does not support this (21, 22, 2). Weakness of the hip is potentially not a cause but more of an effect after acquiring PFPS (2).
Side Note: Posterolateral hip strength is NOT a good indicator of frontal and transverse hip mechanics during running or step-down maneuvers in healthy individuals (2). In other words, having weakness in the hips doesn’t mean you’ll move poorly. Another interesting thing observed in our medical literature is that hip strengthening does NOT improve biomechanics during single leg squat and running activities (2, 4).
These activities improve with cues and biofeedback (mirror feedback) during specific tasks and tend not to improve from task to task (improving a single leg squat does not improve running mechanics) (2, 4). This concept will become very important when we discuss rehabilitation.
Lastly, there are a variety of factors that can lead to knee valgus (motor control, pain, weakness, mobility restriction at the ankle) and if we think valgus is driving pain then we'll have to determine which of these variables is the issue and start working there.
Regardless, hip strengthening has been shown to be an effective treatment for PFPS and even more so when combined with quadriceps strengthening (2, 7, 8). Some authors theorize that hip strengthening improves the PF joint’s capacity indirectly, thus increasing the joint’s ability to handle stress and decrease pain (2, 4).
3: Movement Quality
Femoral internal rotation and tibial external rotation both lateralize the stress to the knee and decrease surface area within the joint to dissipate force. All of these things increase stress to the PF joint. Excessive pronation at the foot (4), lack of ankle dorsiflexion (26, 27) and contralateral hip drop during single leg squatting maneuvers and jumping can all drive abnormal femoral and tibial rotation as well .
People with PFPS had more ipsilateral (same side) trunk lean, contralateral (opposite side) pelvic drop, hip adduction and knee valgus (3) during a single leg squat. In individuals with PFPS, correcting these biomechanical faults can improve their symptoms (2, 10, 14). Having patients go into more knee valgus, hip adduction and foot pronation has been shown to provoke these patient’s knee pain (3). Basically, correcting these movements makes people feel better and worsening these movements creates more knee pain.
It makes sense then that keeping neutral alignment of the PF joint during movement can improve capacity of the knee.
Side Note: Only 50% of patients with PFPS present with these mal-alignment issues (4). This means that there are probably many other factors that contribute to pain besides just altered movement. This is also a potential reason why many athletes can have “poor” mechanics during running and never experience any knee pain. They may have built capacity in other ways and can handle the increased stress without trouble.
As we descend deeper into knee flexion (knee bending) and as the degree of quad contraction increases we increase stress within the PF joint. Having more knee flexion and stronger quad contractions will increase stress in the PF joint. This will become important during rehabilitation when PF joint capacity is limited and we’re attempting to apply the right dosage of exercise to reduce pain and restore homeostasis.
Side Note: Lastly, keep in mind that some of these "abnormal" strategies (hip drop, valgus etc.) occur from knee pain or weakness at the quads (I used parentheses because I think these compensations are completely normal given the situation). The body is attempting NOT to move through the knee but instead from the bigger, stronger and less painful joint above (the hip). So as we attempt to clean these movements up just understand that we're also going to be making the knee joint perform more work.
4: Psychosocial Factors
Dictionary.com describes psychosocial as:
- Relating to the interrelation of social factors and individual thought and behavior
Psychosocial factors are beliefs and social issues that can drive positive or negative behaviors during rehabilitation.
Patellofemoral pain syndrome is correlated with anxiety, depression, fear of movement (kinesiophobia) and catastrophization (2, 25,40). These are known psychosocial factors that can complicate the rehabilitation process. These factors can decrease a patient’s desire to perform movements that improve pain and are also thought to sensitize our nervous system and create more pain.
One example of a catastrophization would be:
“I can’t believe my knee hurts when I try to squat. It will never get better and I’ll never be able to compete in weightlifting ever again”
An example of a negative belief contributing to perpetuation of pain would be:
“Having pain is a sign that my knee is not improving, is getting worse and is probably getting damaged further”
These thoughts and beliefs can and should be addressed through a combination of therapeutic neuroscience education and cognitive behavioral therapy (CBT).
Side Note: Understanding these principles is far beyond the scope of this article. If you'd like more information on therapeutic neuroscience education and CBT then check out Adrian's Louw's "Therapetuic Neuroscience Education and Jason Satterfield's Course on Cognitive Behavioral Therapy.
Lastly, conditions such as anxiety and depression perpetuate the release of stress hormones like cortisol. Cortisol is a hormone that can sensitize your nervous system and increase pain (28) . We know that perceived stress in adolescents correlates with pain levels. (39). Therefore, there is likely a link between the two that should be addressed in those with PFPS.
5: Genetics and Body Mass Index
Now, half of this is either good or bad news. We can’t really pick our parents. Genetically we’re given a specific shape to our patella and trochlear groove. As discussed earlier, this is going to change from person to person. In some people, the fit of the patella and trochlear groove just isn’t great. In some people it is.
The other piece of the equation is body mass index (BMI). Body mass index is the ratio of your height to your weight. If you’re very heavy and short then you’ve got a higher BMI. This is something we can control. Having a higher BMI correlates with patellofemoral pain syndrome in adults only (23). For some reason BMI is not correlated with PFPS in adolescents (23). Either way, it makes sense. The heavier you are, the more stress will go through the PF joint every time you use your lower body.
6. Recovery (Sleep and Nutrition)
When it comes to an overuse injury there are generally two sides of the equation. You've got:
- Total stress thrown at the joint
- The joint's capacity
If the stress exceed's the joint's ability to tolerate load we get breakdown. Another player in the joint's capacity is it's ability to recover. If the joint can recover more quickly then it makes sense that it should be able to handle more stress. The heavy hitters for recovery are going to be sleep and nutrition.
Sleep
Although in it's infancy, sleep and pain are beginning to be found to be tightly correlated in our medical literature. We have research to show that knee pain (especially combined with low back pain) correlates with both reduced sleep duration and quality of sleep. (41). We also know that too much (>9 hours) and too little (<6 hours) sleep directly impact pain levels the following day. (38)
We also have research that poor sleep: (42)
- Increases the risk for new-onset cases of chronic pain in pain free individual
- Worsens the long-term prognosis of existing headache and chronic musculoskeletal pain
While good sleep: (42)
- Appears to improve the long-term prognosis of individuals with tension-type headache, migraine, and chronic musculoskeletal pain
Now, keep in mind that these studies are not strictly in folks with knee pain or even PFPS. Several of these studies are in folks with chronic pain and with headaches. We have to be careful not to immediately apply these results to our patients with PFPS although the link in interesting.
Nutrition
In my opinion nutrition undoubtedly plays a role in pain. However, the interaction between the two has only recently been studied and like with sleep we're still in the infancy of understanding the interaction between the two (and I am admittedly NOT the expert in this regard). Just the interaction between obesity and knee pain is enough to seriously consider nutrition an important player in knee pain. However, we also have some interesting research on nutrition and pain to consider...
One study that reviewed 12 different articles in the Journal of Clinical Medicine (2020) showed that: (43)
- Seven out of nine experimental studies reported a pain-relieving effect of dietary changes
- Protein, fat, and sugar intake were found to be associated with pain intensity and pain threshold
- Chronic pain severity shows a positive relation with fat and sugar intake in osteoarthritis
- Pain threshold shows a positive association with protein intake in fibromyalgia
Just keep in mind that we can't jump to the conclusion that knee pain is directly caused by diet. However, the link between the two is interesting and more research should be performed in the future to learn more.
Keys to Optimize the Health of the PF Joint
So now that we know the factors that influence the PF joint's capacity we can go about improving the joint's health in a systematic format. These go for folks both trying to prevent injury as well as getting out of pain once injury has already occurred. Here are the keys to doing just that:
- Follow proper programming principles minimizing excessive volume in training and spikes in training volume
- Utilize strengthening to the muscles surrounding the knee and hip
- Encourage optimal biomechanics during lifting, running and moving
- Promote a positive psychosocial environment and minimize stress
- Optimize recovery through adequate sleep and nutrition
- Strike the lottery with great genetics
- Keep bodyweight (BMI) in check
Now let’s take this information and bring it back to our runner examples earlier in the article series. If you remember, “runner B” got injured. “Runner B” also had less capacity than runner A. Maybe “runner B”:
- Did not prepare herself to run the marathon as thoroughly as “runner A”
- Had less quadriceps strength than “runner A”
- Had dynamic valgus of the knee during running
- Was dealing with a recent divorce and bout of depression during training and the race
- Has a more shallow trochlear groove than “runner A”
- Was only sleeping 5-6 hours per night
- Was carrying around a few extra pounds more then what is considered a normal BMI
Any of these factors could have decreased her capacity and increased her risk of injury. As you can see, the reason for an injury can come from a variety of places and is probably multi-factorial in nature as well.
It’s often not 1 single factor (technique, strength, mobility) that leads to an injury. All of these factors are probably relevant. We'll delve into these more in a moment but's let's recap what we covered so far.
So to recap:
- Patellofemoral pain syndrome is influenced by our knee’s total “capacity”
- High levels of capacity can buffer against injury
- PF joint capacity is influenced by a variety of factors
- Whether or not you experience knee pain depends on a complex interaction of all of these factors
Explaining Pain to Patients with Patellofemoral Pain
Now, what happens once pain occurs? Based on the theory by Scott Dye, when the capacity of the joint is overcome pain results. Once pain becomes involved our joint capacity lowers and now we can't handle as much activity without pain.
Understanding Pain
I made a few graphs to help understand this concept. Basically, before pain we can perform all types of movement without eliciting any pain. 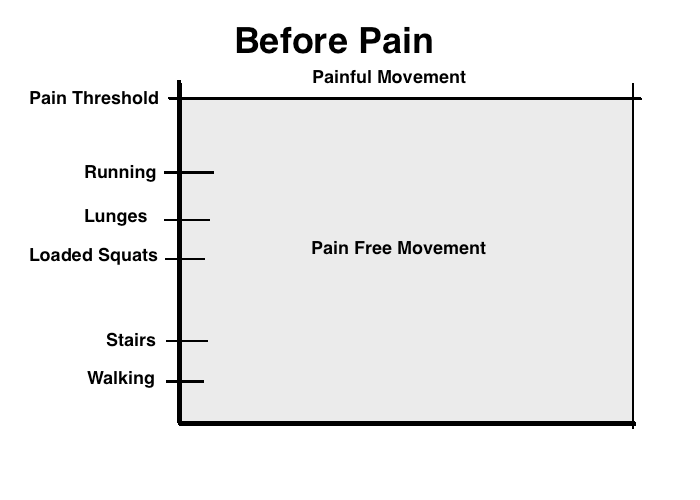 We have adequate capacity to handle all sorts of exercise. Now let's take a look at a knee with PFPS.
We have adequate capacity to handle all sorts of exercise. Now let's take a look at a knee with PFPS.
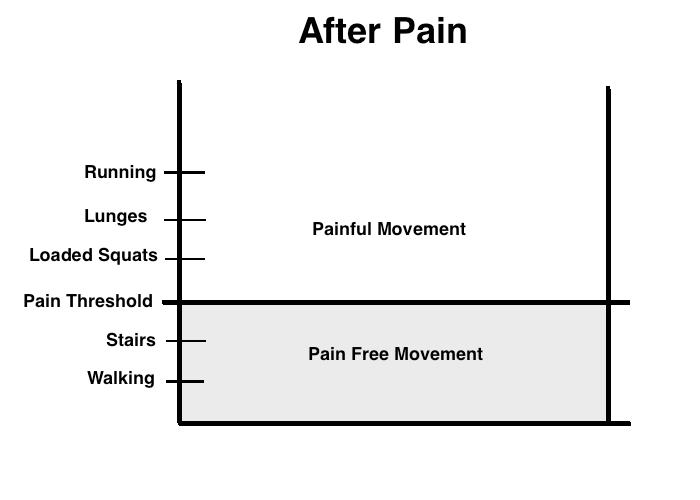
What ends up happening is that we can’t do as much as we could before without experiencing pain. Maybe we can walk and perform stairs without pain but pretty much any lower body training in the gym hurts. In this example we can see that we cant even perform loaded squats without experiencing pain. Our capacity has dropped, and with it our patient's ability to perform the activities they enjoy.
It makes sense, our bodies produce pain in order to protect us after injury (and to prevent future mistakes). In my mind pain is basically our body’s way of telling us to “be careful not to do anything stupid”. After an injury pain exists to keep us safe and to help us regulate the amount of activity we perform so the body can recover.
Exercise Dosage
Pain is also an important guide during our rehabilitation. Exercise stress can cause an injury but it's also what helps us heal after an injury.
What’s interesting about the PF joint is that this initial insult can be prolonged indefinitely if not intervened upon (11) in a large chunk of people. In other words, pain tends to stick around indefinitely unless we do something about it (13).

After injury we need to find the correct dosage of stress in order to make a positive adaptation and improve our knee’s “capacity” back to pre-injury levels. I really the following analogy to help patient's understand this concept.
If you have a headache and take 2 aspirin, the headache will probably go away. We took the proper dosage. If you have a headache and take the entire bottle of aspirin, you’re dead. Wrong dosage. The aspirin wasn’t the wrong choice, the dosage of aspirin was.
The same thing goes for rehabilitation of the PF joint. We need to find the correct dosage of exercise to heal the joint. We already spoke about how patellofemoral pain syndrome tends not to get better in time without intervention (24) and as we just noted toward, too much stress is obviously not good either.
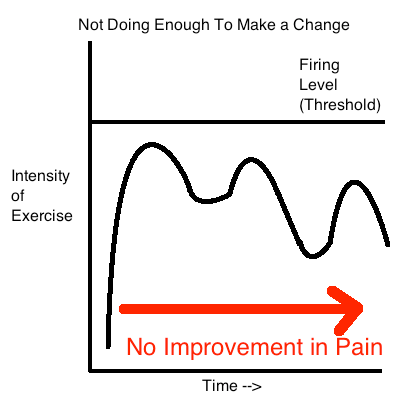
What’s important to understand is that too much stress can end up making the situation worse. However, not enough stress can be equally as bad.
Graph 1
Graph 2
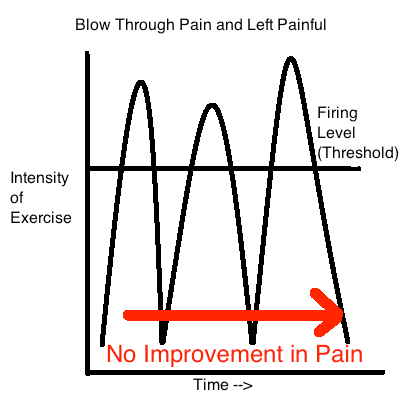
In the third graph you can see the athlete works at their threshold of pain.
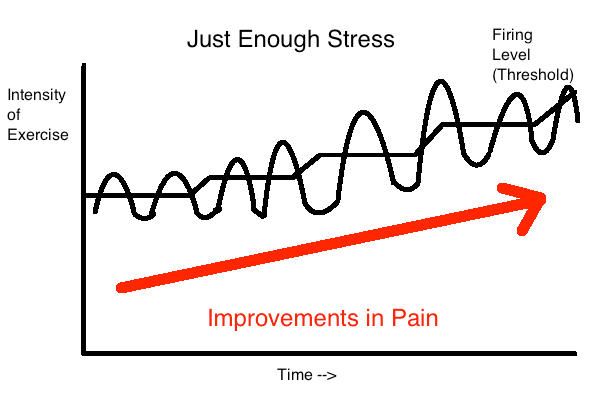
Over time the pain threshold gradually improves. As the threshold improves our athlete works at a slightly higher intensity to reflect the improvements in threshold. Over time this continues and our athlete gradually builds their capacity up again and can do more and more with diminishing levels of pain .
How Much Pain is Appropriate During Exercise?
A key factor in this equation is that our athlete was working with some pain the entire time. There’s quite a bit of research out there showing that working with some pain during rehabilitation exercise is ok and patients do tend to get better over time. Working with some pain during exercise can actually result in faster short term improvements in pain compared to performing rehab exercises without any pain.
Determining how much pain to work with is a very gray area and challenging for therapists and patients alike to determine just how much pain is ok to push through during physical therapy exercises. I wrote an in depth article on how I like figure this out you can access by clicking on this link. My basic principles for pain during physical therapy exercises are:
- Pain should be minimal or at or below a 3/10 on a 0-10 pain scale during exercise
- Pain levels should return to baseline following exercise and the following day
- Pain and function should be improving on a weekly and monthly basis
If these requirements are not being fulfilled we need to change something, the dosage is off. If we’re meeting these requirements, we’re on the right track. It’s honestly an experimental process that we learn more and more about with the passage of time.
Keep in mind that applying rehabilitation exercise properly is like trying to hit a moving target. Exercises difficulty will change over time based on how your body responds.
So to recap:
- The PF joint’s capacity to handle stress decreases after an injury
- Pain is a normal process designed to help protect the body and keep you safe in the future
- Restoring knee capacity and eliminating pain revolves around properly dosing exercise
- Working with small levels of pain can be beneficial to help rehabilitate fully
- How much pain you experience during and after exercise will help guide the intensity of exercise over time
Evidence Based Treatment for Patellofemoral Pain (44)
Patellofemoral pain has been studied extensively and a variety of treatments have been found to be effective for treating patellofemoral pain:
- Education
- Exercise Therapy
- Foot Orthosis
- Patellar taping / mobilization
- “A combination of everything”
1. Education
Education generally consists of information about:
- Basic patellofemoral definition
- Why the knee became irritated
- Pain management strategies
- How to modify physical activity using pacing and load management strategies
- Information on optimal knee alignment during daily tasks
Click HERE to see the exact educational pamphlet given to patients
2. Exercise Therapy
Exercise therapy consists of exercises targeted towards the knee, hip, foot and trunk. Each study used a variety of different exercises and targeted certain areas over others. However, all studies atleast targeted the knee and hip which we have some research to show is superior to knee strength training alone (45). Some studies also included blood flow restriction training as well as aerobic exercise. ( I actually enjoy using BFR on PF pain patients myself...) Read on to see which exercises I like for patellofemoral pain.
3. Foot Orthosis
A prefabricated foot orthoses was found to be helpful in patients with patellofemoral pain. Also keep in mind that patients also received education to go along with the orthoses.
4. Patellar Taping / Mobilization
Patellar taping and mobilizations were also found to be effective for treating patellofemoral pain but also keep in mind that these therapies were also combined with either exercise, orthotics, education or a combination of these other treatments.
Read on to see how I like utilizing some of these treatments for my patients looking to get back to training in the weight room...
Steps to Rehabilitation and Return to Weight Training
Next we'll get into the nitty gritty of rehab and returning to training in the weight room by going through the same principles we touched on earlier. Here's the backbone of PF pain rehab.
- Modify training and lifestyle
- Slowly load and build strength in a graded fashion
- Move right, enhance mobility and decrease pain with self soft tissue work
- Clean up poor psychosocial influences and reduce stress
- Normalize your body mass index (BMI)
- Improve nutrition and sleep
1: Modify training and lifestyle
So after our discussion on pain and restoring homeostasis of the knee it becomes pretty obvious that we have to find the right dosage of stress to get the knee to recover.
The reason I say “stress” is because it’s not just exercise that has to be dosed appropriately in order to get out of pain. Initially our regular activities may have to be dosed as well to reduce some of the stress on the PF joint keeping things irritated. If you perform a manual job or are regularly performing activities such as stair climbing, kneeling or prolonged sitting you may have to modify some of these activities for a period of time before returning back .
If you’re already training (weight training or running) these activities will also have to be modified or eliminated temporarily to respect the capacity of the knee and allow progress.
2: Progressive loading
Once you’ve got your modifications squared away it’s time to start applying stress to the system. In order to slowly increase stress on the PF joint we should keep in mind that increasing knee flexion and quad contraction directly increases stress on the PF joint (2, 4). We can use these principles along with some help from our medical literature on the topic to develop a progressive program for the knee.
How long should a rehabilitation program last?
This program would be at it’s shortest 4 weeks long and at it’s longest 3 months. Most of the research studying PFPS has their participants performing an exercise program for 4-12 weeks with an average frequency of 3 times per week (30, 31). Usually these exercises are progressive in nature to create further adaptations as capacity improves (30, 31).
In the physical therapy realm we often use the term “phases” to help categorize exercise difficulty and total stress. Phase 1 is easiest and as the phases increase the challenge of the program increases progressively. Here are some of my favorite PFPS strengthening exercises in a phased format:
Rehab Exercises:
Each of these phases lasts 2-4 weeks and should last as long as needed to progress to the next phase with minimal pain. Everyone is an individual and some will need more time in each phase then another .
Once you start getting toward the advanced stages of rehabilitation (Phase 3 and beyond) we’ll have to start thinking about the specific demands of the activities you want to get back to. For example:
- Return to running
- Return to weightlifting
- Return to crossfit
Each of these activities stresses the knee in a unique way and rehabilitation will have to reflect these specific needs. The runner will need to start introducing low level plyometrics that stress the knee in a similar way to running with an emphasis on endurance. The weightlifter will have to introduce weighted squats in a gradual fashion slowly increasing depth, load and volume over time.
3: Improve Mobility
Remember we discussed how tightness in the lateral structures of the hip and quadriceps can be related to increased compression within the PF joint and subsequent pain? Well, it’s time to address this.
We want to first assess to see if there are any restrictions in either a Thomas or Ober’s test. Remember that our literature shows that improving these with physical therapy are predictors of who has successful rehabilitation after PFPS (1).
Anterior Hip
Lateral Hip
Side Note: The Ober’s Test was traditional thought to assess limitations of the IT band, TFL and Glute. More recent research has shown that the IT band does not restrict the Ober’s Test but rather the glute medius, glute minimus and the hip capsule. An intervention to address these muscles may be more prudent than the IT band .
Hip Mobility Drills
Side Note: Foam rolling has been shown to improve something called pressure pain threshold (PPT) (32). PPT is basically the amount of pressure the body can handle before pain is experienced. After foam rolling your pain threshold (for pressure) improves. Foam rolling may directly improve pain in the knee through this mechanism. However, I see far too many people who’s rehabilitation program consists exclusively of self soft tissue work and stretching. Keep in mind this is NOT the gold standard when treating knee pain.
After we’ve taken care of these mobility issues it’s also important to address any limitations in mobility that are driving dynamic valgus of the knee during activity. As discussed earlier, limitations in ankle dorsiflexion can cause faulty movement at the knee and hip during step down, jumping and landing activities.
Ankle Dorsiflexion
Ankle Dorsiflexion Mobility Exercises
Tibial Internal Rotation
The other place we'll need mobility to optimize tracking at the PF joint is at the tibio-femoral joint. Check out the video below to learn how to assess this joint with a mobility drill after. Just keep in mind when mobilizing this area you're actively twisting your knee. This mobilization should never be performed with aggression or intensity. Keep it gentle.
4: Improve exercise technique
Next we’ll want to fix up any faulty movement patterns we see during the athlete’s activities. This could be during running, agility d rills, squatting, jumping and landing drills. Remember that hip strength is not necessarily a predictor of who moves poorly and improving hip strength on it’s own does not clean up movement (2, 4).
What does tend to improve an athlete’s movement is either some form of verbal cueing or the use of biofeedback tools like putting a mirror in front of an athlete while performing their sport specific task (2, 4). Also remember that cleaning up someone’s movement during a specific task like a single leg squat will not carry over to correct biomechanics during running (2, 4). Cues and biofeedback need to be utilized during all tasks our athletes wish to get back to .
Some examples would be:
- Cueing your athlete to keep their knees out during a squat
- Putting a mirror in front of an athlete while running and telling them not to allow the knees to come in while running
Also keep in mind that the foot can affect movement up the chain just as an issue at the hip can cause problems down stream. Remember our discussion on excessive foot pronation causing femoral internal rotation:
If you are concerned yourself or an athlete has excessive pronation at the foot (and subtalar joint as discussed in the first article in the series) driving issues at the knee you might have to learn how to correct this with a technique called the short foot:
Once you learn how to create this arch in the foot it can be strengthened through specific exercises. This short foot posture can also be trained through during your normal lower body exercises, which I would recommend doing.
Side Note: Keep in mind that limited ankle dorsiflexion can cause faulty mechanics during squatting and jumping. Also, excessive pronation can alter movement creating poor mechanics at the knee. However, the evidence is mixed in this regard. Some research shows that limited dorsiflexion is correlated to injury, some not and some shows the opposite (more mobility can predict who gets knee pain) (4,9). The same thing goes for pronation, some studies show it is correlated with knee issues and some not (4, 9). I think the take home message is to try and work on the factors you believe may be contributing to poor movement and pain but also don’t assume that having a flat foot or poor ankle mobility will condemn anyone to a future of miserable knee pain. Remember that having pain and injury is multi-factorial and in theory if all other factors are optimized (to improve capacity) you may never have knee pain in the future.
5: Improve psychosocial status
Now, this topic is starting to go beyond the scope of a typical physical therapist’s set of skills. However, it is an important player in terms of rehabilitation and injury prevention. If you believe you’ve got an athlete on your hands that needs more in depth work in this realm, definitely make sure you go see a professional that’s suited for the job.
With that being said, there are some simple things we can focus on to help in this regard (33).
- Identify anxiety and depression and refer out for additional services
- Identify any poor beliefs
- Patient education
- Influence positive beliefs and behaviors through the use of cognitive behavioral therapy (CBT) techniques
- Improve mental health through behavioral strategies
Some inherent conditions that are linked to PFPS are having anxiety and depression. This may be a potential explanation for the increased likelihood of these conditions and PFPS. Any individuals you suspect may have issues with anxiety or depression should see a professional to help in this area.
Poor beliefs are also implicated in individuals with PFPS (2, 25). Poor beliefs include things like a fear of movement, a belief that pain is a sign of more damage to the body, catastrophizations and beliefs that returning back to regular activities will worsen your condition. We have quite a bit of research to show that these beliefs tend to keep people from getting better when attempting to rehabilitate (34, 35), so it becomes our job to help educate folks that this simply isn't the case.
Also keep in mind that poor beliefs can lead to poor behaviors. If an individual believes that knee pain means they should rest the body they may never get moving.
Catastrophization is having an irrational thought that implies something is far worse than it actually is. These are often triggered when athletes feel pain when training in the gym. For an athlete with PFPS a triggering event may be feeling his or her knee pain when squatting in the gym. The ensuing catastrophization may be:
“I can’t believe my knee hurts when I try to squat. It will never get better and I’ll never be able to compete in weightlifting ever again”
When we evaluate the above statement we realize pretty quickly the statement isn’t very factual or logical. PFPS is a condition that gets better with the right rehabilitation and competing in the future is not only a possibility but also much more likely than not being able to compete in the future. Worse yet, these thoughts can spiral out of control and are thought to increase sensitivity of the nervous system and perpetuate pain (36). It's our job to help our patients see this and focus on the positives.
If you have any of these poor beliefs they need to be addressed via education and strategies like cognitive behavioral therapy (CBT). CBT is basically a strategy of disputing negative thoughts that create poor behaviors and perpetuate pain (33, 35). In this way people in pain can be more objective about their pain, more positive about their outcomes and better able to make behavioral changes that lead to improved pain levels. (and generally not freak out about pain in the gym)
6: Improve Body Mass Index (BMI)
Now this one is pretty obvious. The more weight you carry around on a regular basis, the more stress on the knees. Getting on a solid nutrition and exercise program can help out in this regard.
7: Improve Sleep and Nutrition
For the reasons discussed previously it's a no brainer we should be trying our best to get a full 8 hours of sleep at night to improve our nutrition.
So to recap:
- Modify training and lifestyle activities to respect the joint’s limited capacity after an injury
- Start gradually loading the hip and knee through a progressive strengthening program
- Identify and correct soft tissue and mobility limitations in the ankle, quads, glutes and hip flexors
- Reduce pain levels using soft tissue techniques like foam rollers
- Correct any movement faults through biofeedback and verbal cues.
- Clean up poor psychosocial influences using therapeutic neuroscience education and CBT
- Normalize your BMI to reduce stress on the knee
- Improve stress levels, improve sleep quality and nutrition as icing on the cake
That’s it guys! I hope you enjoyed this guide. If you found it useful please share it with anyone else you think could benefit from it. Making this article was a colossal undertaking for me (took a few months of research, writing, filming and editing and refining over the last few years and I've also been updating it yearly as well!). Thank you for taking the time to read it. Hopefully it helps you with your understanding of patellofemoral pain syndrome!
My knee caps need a break,
Dan Pope DPT, OCS, CSCS
Works Cited:
- Current Concepts and Treatment of Patellofemoral Compressive Issues IJSPT 2016 https://www.ncbi.nlm.nih.gov/pubmed/27904792
- Current Concepts in Biomechanical Interventions for Patellofemoral Pain IJSPT 2016 https://www.ncbi.nlm.nih.gov/pubmed/27904791
- Examination of the Patellofemoral Joint IJSPT 2016 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5095938/
- Biomechanics and pathomechanics of the Patellofemoral Joint IJSPT 2016 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5095937/
- Salsich GB, Perman WH . Patellofemoral joint contact area is influenced by tibiofemoral rotation alignment in individuals who have patellofemoral pain. J Orthop Sports Phys Ther. 2007;37(9):521-528.
- Tibiofemoral and Patellofemoral Mechanics are Altered at Small Knee Flexion Angles in People with Patellofemoral Pain https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3425715/
- Kay M Crossley, Marienke van Middelkoop, Michael J Callaghan, Natalie J Collins, Michael Skovdal Rathleff, Christian J Barton, 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 2: recommended physical interventions (exercise, taping, bracing, foot orthoses and combined interventions) BJSM http://bjsm.bmj.com/content/early/2016/05/31/bjsports-2016-096268
- Christian John Barton, Simon Lack, Steph Hemmings, Saad Tufail, Dylan Morrissey, The ‘Best Practice Guide to Conservative Management of Patellofemoral Pain’: incorporating level 1 evidence with expert clinical reasoning BJSM 2015http://bjsm.bmj.com/content/49/14/923#T
- Patellofemoral pain syndrome and its association with hip, ankle, and foot function in 16- to 18-year-old high school students: a single-blind case-control study. https://www.ncbi.nlm.nih.gov/pubmed/21622633
- Factors associated with patellofemoral pain syndrome: a systematic review. BJSM 2013 https://www.ncbi.nlm.nih.gov/pubmed/22815424
- The Pathophysiology of Patellofemoral Pain Syndrome – Scott Dye http://prdupl02.ynet.co.il/ForumFiles_2/19447772.pdf
- Hartmann, H., Wirth, K., & Klusemann, M . (2013). Analysis of the Load on the Knee Joint and Vertebral Column with Changes in Squatting Depth and Weight Load. Sports Med.
- 2016 Patellofemoral pain consensus statement from the 4th International Patellofemoral Pain Research Retreat, Manchester. Part 1: Terminology, definitions, clinical examination, natural history, patellofemoral osteoarthritis and patient-reported outcome measures” in Br J Sports Med, volume 50 on page 839.
- Trunk and lower extremity segment kinematics and their relationship to pain following movement instruction during a single-leg squat in females with dynamic knee valgus and patellofemoral pain. 2015 https://www.ncbi.nlm.nih.gov/pubmed/24836048
- The Basic Science of Articular Cartilage – Sports Health 2009 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3445147/
- Patellofemoral joint kinetics while squatting with and without an external load . JOSPT 2002 https://www.ncbi.nlm.nih.gov/pubmed/11949662
- The Development and Application of an Injury Prediction Model for Noncontact, Soft-Tissue Injuries in Elite Collision Sport Athletes. (n.d.). Retrieved August 01, 2016, from https://www.researchgate.net/publication/46288877_The_Development_and_Application_of_an_Injury_Prediction_Model_for_Noncontact_Soft-Tissue_Injuries_in_Elite_Collision_Sport_Athletes
- Relationship Between Training Load and Injury in Professional Rugby League https://www.researchgate.net/profile/Tim_Gabbett/publication/49775412_Relationship_between_training_load_and_injury_in_professional_rugby_league_players/links/551894590cf2d70ee27b41ad.pdf
- Training and game loads and injury risk in elite Australian footballers. (n.d.). Retrieved from https://www.researchgate.net/profile/Brent_Rogalski/publication/234699103_Training_and_game_loads_and_injury_risk_in_elite_Australian_footballers/links/53dadd6b0cf2a19eee8b3f9f.pdf
- The acute:chronic workload ratio predicts injury: high chronic workload may decrease injury risk in elite rugby league players. Retrieved from http://bjsm.bmj.com/content/50/4/231 Hulin, Gabbett, Lawson, Caputi, Sampson
- Prospective Predictors of Patellofemoral Pain Syndrome: A Systematic Review With Meta-analysis . Sports Health 2012
https://www.ncbi.nlm.nih.gov/pubmed/23016077 - Factors associated with patellofemoral pain syndrome: a systematic review. BJSM 2013 https://www.ncbi.nlm.nih.gov/pubmed/22815424
- Is body mass index associated with patellofemoral pain and patellofemoral osteoarthritis? A systematic review and meta-regression and analysis. BJSM 2017 https://www.ncbi.nlm.nih.gov/pubmed/27927675
- Is Knee Pain During Adolescence a Self-limiting Condition? Prognosis of Patellofemoral Pain and Other Types of Knee Pain. AJSM 2016 https://www.ncbi.nlm.nih.gov/pubmed/26792702
- The psychological features of patellofemoral pain: a systematic review. BJSM 2017 https://www.ncbi.nlm.nih.gov/pubmed/28320733
- The Association of Ankle Dorsiflexion Range of Motion With Hip and Knee Kinematics During the Lateral Step-down Test. JOSPT 2016
https://www.ncbi.nlm.nih.gov/pubmed/27686412 - The effect of reduced ankle dorsiflexion on lower extremity mechanics during landing: A systematic review Journal Sci Med Sport 2017 https://www.ncbi.nlm.nih.gov/pubmed/26117159
- Stress and Your Body: The Great Courses by Robert Sapolsky
- Effectiveness of Manual Therapy on Pain and Self-Reported Function in Individuals With Patellofemoral Pain: Systematic Review and Meta-Analysis JOSPT 2018 https://www.jospt.org/doi/pdf/10.2519/jospt.2018.7243
- Effectiveness of hip muscle strengthening in patellofemoral pain syndrome patients: a systematic review https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4518569/
- Exercise for treating patellofemoral pain syndrome: an abridged version of Cochrane systematic review. https://www.ncbi.nlm.nih.gov/pubmed/26158920 Cochrane 2016
- Differences in pressure pain threshold among men and women after foam rolling. https://www.ncbi.nlm.nih.gov/pubmed/29037655
- Managing Chronic Pain – John Otis: Treatments that Work
- A prospective study predicting the outcome of chronic low back pain and physical therapy: the role of fear-avoidance beliefs and extraspinal painhttps://www.ncbi.nlm.nih.gov/pubmed/26995499
- Nonspecific Low Back Pain and Return to Work https://www.aafp.org/afp/2007/1115/p1497.html#sec-7
- Therapeutic Neuroscience Education – Adriaan Louw
- Ulrika Aasa et al. Injuries among weightlifters and powerlifters: a systematic review BJSM 2017
- Capin JJ, Snyder-Mackler L. The current management of patients with patellofemoral pain from the physical therapist's perspective. Ann Jt. 2018;3:40. doi:10.21037/aoj.2018.04.11
- Østerås B, Sigmundsson H, Haga M. Perceived stress and musculoskeletal pain are prevalent and significantly associated in adolescents: an epidemiological cross-sectional study. BMC Public Health. 2015;15:1081. Published 2015 Oct 23. doi:10.1186/s12889-015-2414-x
- Maclachlan LR, Collins NJ, Matthews MLG, Hodges PW, Vicenzino B. The psychological features of patellofemoral pain: a systematic review. Br J Sports Med. 2017;51(9):732-742. doi:10.1136/bjsports-2016-096705
- Murase K, Tabara Y, Ito H, et al. Knee Pain and Low Back Pain Additively Disturb Sleep in the General Population: A Cross-Sectional Analysis of the Nagahama Study. PLoS One. 2015;10(10):e0140058. Published 2015 Oct 7. doi:10.1371/journal.pone.0140058
- Finan PH, Goodin BR, Smith MT. The association of sleep and pain: an update and a path forward. J Pain. 2013;14(12):1539-1552. doi:10.1016/j.jpain.2013.08.007
- Elma Ö, Yilmaz ST, Deliens T, et al. Do Nutritional Factors Interact with Chronic Musculoskeletal Pain? A Systematic Review. J Clin Med. 2020;9(3):702. Published 2020 Mar 5. doi:10.3390/jcm9030702
- Winters M, Holden S, Lura CB, et al. Comparative effectiveness of treatments for patellofemoral pain: a living systematic review with network meta-analysis [published online ahead of print, 2020 Oct 26]. Br J Sports Med. 2020;55(7):369-377. doi:10.1136/bjsports-2020-102819
- Nascimento LR, Teixeira-Salmela LF, Souza RB, Resende RA. Hip and Knee Strengthening Is More Effective Than Knee Strengthening Alone for Reducing Pain and Improving Activity in Individuals With Patellofemoral Pain: A Systematic Review With Meta-analysis. J Orthop Sports Phys Ther. 2018 Jan;48(1):19-31. doi: 10.2519/jospt.2018.7365. Epub 2017 Oct 15. PMID: 29034800.
- van Middelkoop M, van der Heijden RA, Bierma-Zeinstra SMA. Characteristics and Outcome of Patellofemoral Pain in Adolescents: Do They Differ From Adults? J Orthop Sports Phys Ther. 2017 Oct;47(10):801-805. doi: 10.2519/jospt.2017.7326. Epub 2017 Sep 4. PMID: 28870143.
- Neal BS, Lack SD, Lankhorst NE, et al Risk factors for patellofemoral pain: a systematic review and meta-analysis British Journal of Sports Medicine 2019;53:270-281.
- PFPS X-ray Image: Source: Attribution: Jmarchn / CC BY-SA (https://creativecommons.org/licenses/by-sa/3.0) Edited by fitness pain free LLC
- INJURY RISK IS ALTERED BY PREVIOUS INJURY: A SYSTEMATIC REVIEW OF THE LITERATURE AND PRESENTATION OF CAUSATIVE NEUROMUSCULAR FACTORS Int J Sports Phys Ther. 2014 Oct; 9(5): 583–595. Jessica Fulton, PT, DPT, HFS,1 Kathryn Wright, PT, DPT,1 Margaret Kelly, PT, DPT, CSCS,1 Britanee Zebrosky, PT, DPT, CSCS,1 Matthew Zanis, PT, DPT, ATC, CSCS,1 Corey Drvol, PT, DPT,1 and Robert Butler, PT, PhD1
- Chronic lack of sleep is associated with increased sports injuries in adolescent athletes. J Pediatr Orthop. 2014 Mar;34(2):129-33. Milewski MD1, Skaggs DL, Bishop GA, Pace JL, Ibrahim DA, Wren TA, Barzdukas A
- Psychological predictors of injury among elite athletes S A Galambos1, P C Terry1, G M Moyle1, S A Locke1 BJSM 2005
- Barber Foss KD, Myer GD, Chen SS, Hewett TE. Expected prevalence from the differential diagnosis of anterior knee pain in adolescent female athletes during preparticipation screening. J Athl Train. 2012;47(5):519-524. doi:10.4085/1062-6050-47.5.01
- Maclachlan LR, Collins NJ, Matthews ML, et al The psychological features of patellofemoral pain: a systematic review British Journal of Sports Medicine 2017;51:732-742.
- Winters M, Holden S, Lura CB, et al. Comparative effectiveness of treatments for patellofemoral pain: a living systematic review with network meta-analysis [published online ahead of print, 2020 Oct 26]. Br J Sports Med. 2020;55(7):369-377. doi:10.1136/bjsports-2020-102819
- Nascimento LR, Teixeira-Salmela LF, Souza RB, Resende RA. Hip and Knee Strengthening Is More Effective Than Knee Strengthening Alone for Reducing Pain and Improving Activity in Individuals With Patellofemoral Pain: A Systematic Review With Meta-analysis. J Orthop Sports Phys Ther. 2018 Jan;48(1):19-31. doi: 10.2519/jospt.2018.7365. Epub 2017 Oct 15. PMID: 29034800.